 By Michael Sciara, Guest Columnist
By Michael Sciara, Guest Columnist
Superstorm Sandy exposed critical weaknesses in the Resiliency of health care systems throughout the North East.
This was especially true for coastal areas and other areas prone to river flooding and flash flooding in New York City, Long Island and New Jersey.
NYC fared fairly well during Sandy, although there were Hospital, Long Term Care and Adult Care Facility closures. This was the case because the Health Care system had excess surge capacity and unaffected neighboring facilities had the ability to “Pick up the Slack”.
The nightmare scenario involves a series of catastrophic events occurring simultaneously during a severe weather event which would significantly reduce an impacted health system’s excess capacity. This becomes more likely as the nexus of health services shifts to community based/ambulatory facilities, reducing the reliance on hospitals. There are many community health centers that took months to reopen after Sandy. Some never reopened.
In the aftermath of Sandy, NYC led the charge in taking a hard look at the planning of new health facilities and improving the resiliency of existing facilities. This effort, known as the Special Initiative for Rebuilding and Resiliency or (SIRR), had input from FEMA, the American Institute of Architects (AIA), the US Green Building Council (USGBC), the NYC Building Department and many other experts in disaster preparedness and recovery.
In August of 2013, the New York State Department of Health issued Draft Construction Resiliency Standards which embraced and in some cases exceed those of NYC’s SIRR.
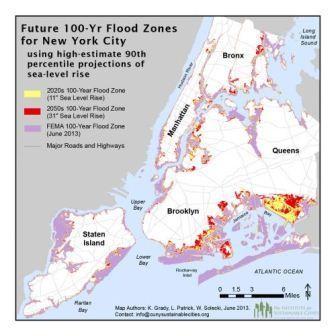 FEMA (The Federal Emergency Management Agency) publishes Flood Insurance Rate Maps (FIRM) for the United States. These maps establish and delineate historical floodplain boundaries and peak flood elevations (relative to mean sea level). Essentially these maps establish the relative likelihood of a given area to flood. For example, if a property is located in a “100-year Flood Zone” (a Special Flood Hazard Area), that property has a 1% chance of experiencing a flood in a given year. A parcel in a 500-year Flood Zone has a 0.2% chance of flooding in a given year. The FIRM maps for New York City are in the process of being modified. The current iteration (available on-line) are called “Work Maps”, but these are subject to change. Special Flood Hazard Areas have a designation of “A” or “V” on the FIRM maps.
FEMA (The Federal Emergency Management Agency) publishes Flood Insurance Rate Maps (FIRM) for the United States. These maps establish and delineate historical floodplain boundaries and peak flood elevations (relative to mean sea level). Essentially these maps establish the relative likelihood of a given area to flood. For example, if a property is located in a “100-year Flood Zone” (a Special Flood Hazard Area), that property has a 1% chance of experiencing a flood in a given year. A parcel in a 500-year Flood Zone has a 0.2% chance of flooding in a given year. The FIRM maps for New York City are in the process of being modified. The current iteration (available on-line) are called “Work Maps”, but these are subject to change. Special Flood Hazard Areas have a designation of “A” or “V” on the FIRM maps.
 Building Codes have required flood mitigation measures to the 100-year floodplain level for many years. It is the opinion of many experts that global warming and other climatic factors will continue to increase the likelihood of severe weather events. Many feel that the bar should be set at the 500-year floodplain. Taking a “Best Practices” approach, several recently constructed major health facilities in New York State have voluntarily been designed to the “500-year Standard”.
Building Codes have required flood mitigation measures to the 100-year floodplain level for many years. It is the opinion of many experts that global warming and other climatic factors will continue to increase the likelihood of severe weather events. Many feel that the bar should be set at the 500-year floodplain. Taking a “Best Practices” approach, several recently constructed major health facilities in New York State have voluntarily been designed to the “500-year Standard”.
NYC is not willing to wait for a “Best Practices” approach to flood mitigation to take hold. As such, the NYC Construction Codes will be amended to require new and existing Health Care facilities to take action to ensure that critical building systems are physically protected from extreme weather impact.
New Hospitals (and substantial improvements to existing facilities) in special flood hazard areas must be designed to the 500-year Standard. Existing hospitals must be retrofitted so that critical equipment is raised above the 500-year floodplain or that spaces containing such equipment be dry flood proofed. Emergency generators must have pre-connections for temporary external generators.
New Nursing Homes (and substantial improvements to existing facilities) in special flood hazard areas must also be constructed with additional resiliency measures for their emergency power systems including a pre-connection for an external generator. The DOH Draft Resiliency Standards recommend that new nursing homes be designed to meet the 500-year floodplain standard. This exceeds NYC’s 100-year requirement. NYC will also require that a minimum, new adult homes install a pre-connection to an external stand-by generator (and maintain a current contract with a generator provider).
Existing Nursing Homes in NYC Flood Hazard Areas must be retrofitted to the 100-year standard by 2030 and must file an interim report by 2020 certifying compliance or submit an Affidavit describing a plan of compliance by 2030. Requirements include protection of electrical equipment, emergency power systems and domestic water pumps. NYC may make funding available to offset some retrofit costs.
Existing NYC Adult Homes in Flood Hazard Areas must also become more resilient by 2030. Electrical equipment must be elevated or protected and an emergency generator pre-connection must be installed. Interim progress reports are due by 2020.
 NYC will encourage and support several best practices through mitigation grants, loans and tax incentives. These include; increasing air conditioning capacity of Nursing Homes and Adult Homes (increased emergency power capacity), harden the resiliency of Primary Care and Mental Health Clinics, encourage telecommunications and medical records resiliency. The support of these best practices is mirrored by the DOH Draft Resiliency Construction Standards. DOH is likely to require that CON applicants for Community Based Health Care Centers demonstrate resiliency as a condition of approval.
NYC will encourage and support several best practices through mitigation grants, loans and tax incentives. These include; increasing air conditioning capacity of Nursing Homes and Adult Homes (increased emergency power capacity), harden the resiliency of Primary Care and Mental Health Clinics, encourage telecommunications and medical records resiliency. The support of these best practices is mirrored by the DOH Draft Resiliency Construction Standards. DOH is likely to require that CON applicants for Community Based Health Care Centers demonstrate resiliency as a condition of approval.
It is generally acknowledged that the retrofitting of existing health facilities is at best very expensive and at worst, logistically impossible. Recognizing this, the AIA recommended that the NYC Code revisions include some mechanism for non-compliance such as an alternate strategy of evacuation to a protected alternate facility with excess capacity. It is not certain whether the final NYC text will include such exceptions.
The DOH Draft Resiliency Construction Standards are not mandating the retrofit of facilities outside of Special Flood Hazard Areas. However, they do recommend that all facilities undertake resiliency assessment be completed and presented to the Board of Trustees for consideration as they approve Long Term Capital plans. The AIA, in its report to NYC, also recommends that a vulnerability assessment be the first step in resiliency planning and that the City Council should enact a law requiring these assessments.
Another key recommendation of the AIA is that building wind design requirements should be upgraded to ASCE/SEI 7-10. This professional reference standard requires that critical buildings such as Hospitals be constructed to resist higher wind velocities than the current standard. It is unclear at this time whether NYC will adopt this recommendation.
“Resiliency” will be one of the most used words in the Facilities, Construction and Health Care lexicons over the next 15 years. Once again the Health Care industry will have to adapt and re-invent itself.
Recommendations of the DOH Ad Hoc Advisory Committee on Environmental Construction Standards – August 2013 (Abbreviated Summary of Major Recommendations):
1. Health Facilities should be designed & constructed to maintain life safety and provide services if flood waters reach the 500-year crest level. (Regulatory Change)
2. Health Care Providers should include Resiliency and Storm Mitigation activities in long term capital plans for physical plant improvements. (Best Practice Recommendation)
- Require installation of flood resistant emergency generators and fuel supplies or pre-connections for external generators
- Require generators and fuel pumps to always be accessible
- All emergency generators shall have pre-connections
- Require pre-connections for temporary boilers and chillers if equipment is located below the design flood elevation
- Require HVAC for inpatient units to be operational during power outages by installing extra generator capacity
3. Apply best practice recommendations to all New Health Facilities including Ambulatory and Out Patient facilities.
4. Harden IT infrastructure to insure patient information remains accessible even if a facility needs to evacuate.
5. Voluntary adoption of best practices by existing Article 28 providers.
- Conduct facility resiliency assessment
- Create a phased plan of investments to improve resiliency
- Present plan to the Board of Trustees for consideration
Resiliency Definitions:
- Dry Floodproofing: A combination of design modifications that results in a building or structure, including the attendant utility and sanitary facilities, being water tight with walls substantially impermeable to the passage of water and with structural components having the capacity to resist loads as identified in ASCE7 code.
- Wet Floodproofing: The use of certain materials/finishes (and the avoidance of certain materials/finishes) below the design flood elevation to reduce the likelihood of mold growth.
- Avoid – Carpeting, Dry Wall, Plaster, Hollow Concrete Block, Wood, Plywood, Particle Board, Other materials with voids and open cells
- Use – Concrete (floors and partitions), Solid Concrete Block (partitions), Ceramic and Quarry Title (floor & wall finish), Terrazzo Flooring, Stainless Steel (casework), Metals (doors, etc.)
- Special Flood Hazard Area: An area delineated on the FEMA Flood Insurance Rate Maps (FIRM) with the letter designation “A” or “V”. Also referred to as a “100-year Flood Zone”.
- Resiliency: The ability of systems and infrastructure to resist, absorb and recover from the impacts of a severe weather event.
- Hardening: Physical Modifications to in-place construction and infrastructure to increase its level of resiliency.
- Substantial Improvement: (NY State Building Code)
- “For the purpose of determining compliance with the flood provisions of this code, any repair, alteration, addition, or improvement of a building or structure, the cost of which equals or exceeds 50 percent of the market value of the structure, before the improvement or repair is started. If the structure has sustained substantial damage, any repairs are considered substantial improvement regardless of the actual repair work performed.”
7. Substantial Improvement: (NYC Building Code)
- “Any repair, reconstruction, alteration, or improvement of a building, the cost of which equals or exceeds fifty percent of its market value either:”
- before the alteration, improvement or repair is started, or
- if the building has been damaged and is being restored before such damage occurred.
For the purpose of this definition, “substantial improvement” is considered to occur when the first alteration of any wall, ceiling, floor or other structural parts of the building commences, whether or not the alteration affects the external dimensions of the building. The term “substantial improvement” does not, however, include either:
- any project for improvement of a building to comply with state or local health, sanitary or safety code specifications which are solely necessary to assure safe conditions, or
- any alteration of a building designated as worthy of preservation because of historic or architectural importance, or a building within an area so designated by the Landmarks Preservation Commission, or listed on the National Register of Historic Places or State Inventory of Historic Places.”
 Michael A. Sciara, AIA is a registered architect with John W. Baumgarten Architects, P.C. in Jericho, NY, specializing in Article 28-Compliancy. The firm seeks to educate and inform the industry with its knowledge of the stringent State-mandated regulations that are placed on facilities. www.jwbarch.com (516) 457-6583.
Michael A. Sciara, AIA is a registered architect with John W. Baumgarten Architects, P.C. in Jericho, NY, specializing in Article 28-Compliancy. The firm seeks to educate and inform the industry with its knowledge of the stringent State-mandated regulations that are placed on facilities. www.jwbarch.com (516) 457-6583.
Discover more from Helping NYC & Long Island Commercial Tenants, Owners, and Developers
Subscribe to get the latest posts sent to your email.